




FUNCTIONS TESTING AND LEAKAGE CURRENT MEASUREMENT PER IEC 60601 AND IEC 62353
HF SURGERY IN THE FIELD OF MEDICINE
During high-frequency surgery (hereinafter referred to as HF surgery), high-frequency alternating current is passed through the human body in order to selectively damage or cut tissue by means of the resulting heat. Diathermy or electrocauterization (from the Greek kaustos for “burnt”) is a surgical method for cutting through tissue structures or for entirely removing body tissue (cauterization) using an electrocauterizer. A significant advantage as compared with conventional incision techniques using a scalpel is that bleeding can be stopped at the same time the incision is made by sealing off the affected vessels. The devices used for this purpose are also known as electric scalpels.
When resecting malignant tumors, use of an electric scalpel close to the tumor should be avoided because the pathologist is unable to assess the burned cut surfaces, and thus can’t determine whether or not the tumor has been fully removed (in sano).
HF electrosurgery is based on Joule’s law. Three different effects occur when electric current flows through the human body:
- Nerve stimulation
- Electrolysis
- Joule’s heat
Heat is taken advantage of in high-frequency surgery. Electrolysis and nerve stimulation only occur to a minimal extent with high frequency alternating current.

HF Surgery in the Operating Room (photo: Medkoh Surgical Instruments)
DEFINITION AND FUNCTION
Electrocauterization generates heat by passing electricity through a wire.
In the case of electrosurgery, heat is generated by passing current through human body tissue via two electrodes.
HF SURGERY is often called diathermy, which comes from the Greek and means “to warm through”:
Dia – through
Therme – warmth
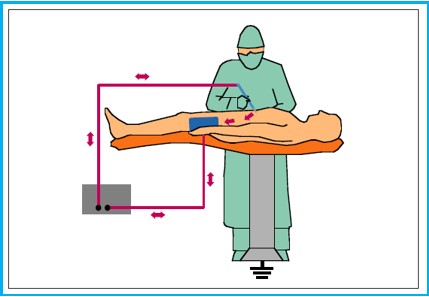
The Concept of Monopolar HF Surgery
The thermal effect is triggered by high-frequency alternating current with frequencies ranging from 300 kHz to 2 MHz. Electrical power of up to 400 W is applied to the tissue under treatment, where thermal effects occur due to the tissue’s resistance. The degree of heating depends on the resistance of the tissue, exposure time and current density. The higher the specific resistance in the tissue, the greater the power input.
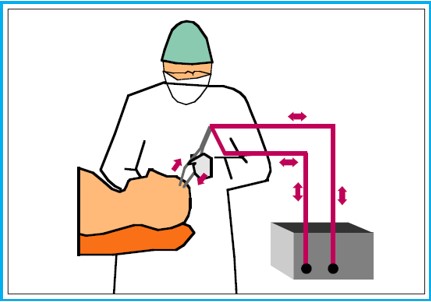
The Concept of Bipolar HF Surgery
Monopolar electrosurgery is most common, in which case the patient’s body completes the circuit. The active electrode (b) is located at the surgical site – represented by a small puncture probe. High current density at the tip generates intense heat (current density is greatest at the tip of a needle). The return electrode (a) has a larger surface area and is located at a different point on the patient (low current density).
Bipolar electrosurgery is performed at the surgical site by the means of the active and the return electrode – usually represented by forceps.
The tissue between the electrodes completes the circuit, thus creating a conducting path at the surgical site. No patient return electrode is required. It should be noted that current flows in both directions.
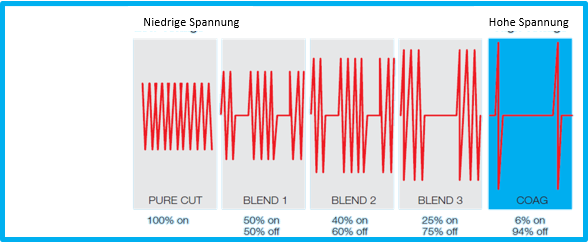
WAVEFORMS
Electrosurgery works with frequencies well above the depolarization threshold of 10 kHz. This prevents excessive neuromuscular stimulation as well as the high risk of electric shock due to the flow of current, and eliminates the possibility of neuromuscular and cardiac dysfunction.
There are three types of waveforms, namely cut, coagulation and blend current.
The Concept of Bipolar HF Surgery
Cut current uses an uninterrupted, pure waveform with high average power and high current density. Coagulation current involves intermittent bursts of attenuated sinewaves. Blend current involves a duty cycle modification and works with voltages between those of cut and coagulation current.
During production, manufacturers of HF surgical equipment must adhere to the strict design conditions set forth in IEC 60601-2-2. This ensures that the equipment is safe for operators and patients, and that injuries and damage are excluded when used properly. Periodic performance and safety testing is required at regular intervals – typically every 6 to 12 months.
Testing typically includes:
- Visual inspection
- Low-frequency electrical safety testing including leakage current up to 1 kHz
- Output power testing at different levels for various loads (load curves)
- Measurement of high-frequency leakage current
- Testing of the patient return electrode and its monitoring
As a rule, test instruments for electrosurgical equipment have to be capable of executing a variety of functions. Automatic test sequences are also required in addition to the necessary measurements. Simulation of a wide variety of patient types and automatic generation of error scenarios permit comprehensive testing of a considerable range of functions and safety aspects. ESU analyzers can be used to test contact quality monitoring systems – either automatically or manually.

SECULIFE ES PRIME Analyzer for HF Surgery
POWER MEASUREMENT
According to IEC 60601-2-2, multiple load resistances must be measured as a function of output power when testing high-frequency surgical equipment, thus making it possible to record so-called power curves.
Testing with at least five different external load resistors is recommended.
Monopolar outputs:
100, 200, 500, 1000 and 2000 Ω
Bipolar outputs
10, 50, 200, 500 and 1000 Ω
As a rule, precision external resistors (1% tolerance range) and a broadband toroidal current transformer are used to this end.

SECULIFE ES PRIME Analyzer for HF Surgery
The current transformer senses the HF current and indicates an output voltage proportional to it. The current is converted to a predefined ratio and transferred to the ESU analyzer. The ESU analyzer displays measurement data such as current, voltage, power, peak voltage and crest factor at the monitor screen. The crest factor, also known as the peak factor, describes the ratio of the peak value to the RMS value of an alternating quantity.
TESTING THE NEUTRAL ELECTRODE / REM
The so-called neutral electrode in split configuration ensures that the electrosurgical generator triggers an alarm and/or reduces output power in the event of poor contact or no contact at all.
Various values are simulated via an internal or external resistance decade – from short circuiting the neutral electrode with 5 to 15 Ω right on up to interruption or poor neutral electrode contact with less than roughly 200 Ω.
Checking for correct operation of contact quality monitoring systems in HF surgical equipment is a very important part of testing in order to protect patients from injury.
Split Neutral Electrode
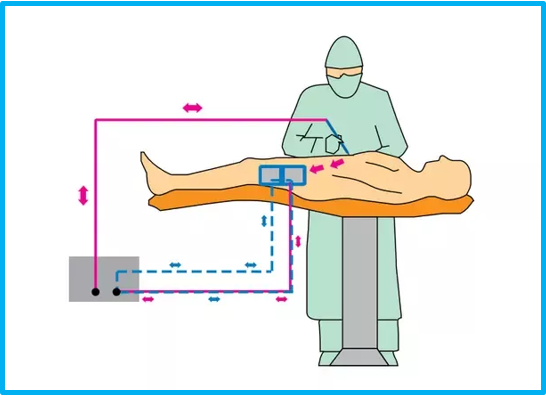
MEASURING HF LEAKAGE CURRENT
At frequencies of greater than 400 kHz, the electric current tends to scatter and may flow from the active electrode through an insulator to another nearby conductor. This effect is known as capacitive coupling and can lead to impaired functionality, as well as possible injury to the patient. Coupling occurs when HF energy induces a secondary, unintended current path through a conductive surface. These conductive materials are not necessarily conductive parts of the device, but rather, for example, human tissue.
The high-frequency leakage current test measures high-frequency leakage current in various test configurations and compares the results to a user-selected pass/fail value when using an electrosurgical analyzer.
Leakage current 1: This active electrode to ground leakage current test is specified by the IEC and is used to test HF leakage current to ground at the isolated output of a type CF electrosurgical generator using a single active or neutral cable.
Leakage current 2: This leakage current test for type BF grounded devices (load between the electrodes) is used to test HF leakage current to ground at the grounded output of a type BF electrosurgical generator using the active output.
Leakage current 3: This leakage current test for type BF grounded devices (load from active electrode to ground) is used to test HF leakage current to ground at the grounded output of a type BF electrosurgical generator using the active output.
These tests comply with the requirements specified in IEC 601.2.2, figure 104 in section 19.101b and section 19.102, on which ANSI/AAMI HF18-2001 is also based.













